Why cognitive bias persists in clinical decision making

Cognitive bias in clinical decision making is one of the most extensively studied problems in medicine, and one of the least solved. Clinicians have been taught about anchoring, availability bias, and premature closure for decades. Diagnostic error rates have not meaningfully improved in response.
The reason is structural rather than motivational. Cognitive biases operate in System 1 processing, which is fast, automatic, and largely inaccessible to voluntary oversight. The knowledge a clinician holds about those biases lives in System 2, which is slow, deliberate, and only partially available under the time pressure and cognitive load of real clinical work. Awareness of a bias and protection from it are not the same thing. Understanding why they are different changes what it is reasonable to ask clinical training to do.
A clinician who can name every cognitive bias that affects diagnosis is not meaningfully protected from any of them, because the knowledge that would need to intervene operates at a different level than the bias does.
Why does knowing about cognitive bias not protect clinicians from it?
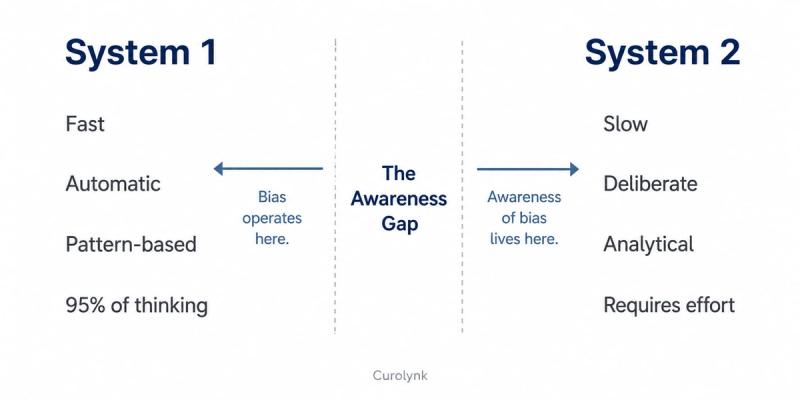
Cognitive biases are not errors of knowledge. They are features of the same System 1 processing that makes experienced clinicians fast and accurate. Daniel Kahneman's dual process framework distinguishes System 1, which is intuitive, pattern-based, and automatic, from System 2, which is analytical, deliberate, and effortful. In clinical practice, System 1 dominates. Cognitive psychologists estimate that clinicians, like all people, spend approximately 95 percent of their thinking in System 1 mode, including under the conditions that define real clinical environments: time pressure, high patient volume, incomplete information, and cognitive fatigue.
Cognitive biases emerge directly from System 1 processing. Anchoring bias, where a clinician over-weights the first piece of information they receive, is System 1 pattern-matching doing its job efficiently. Availability bias, where recent or emotionally vivid cases distort probability judgments, is System 1 drawing on its most accessible examples. Premature closure, where the diagnostic search ends once a plausible explanation appears, is System 1 resolving ambiguity quickly so the clinician can act.
Knowing that these biases exist is a System 2 activity. It requires deliberate, conscious reflection on a reasoning process that is already complete by the time reflection begins. By the time a clinician consciously considers whether they might be anchoring, the anchored judgment has already shaped what evidence they are attending to and what they are discounting. Awareness arrives after the bias has acted. This is the structural mismatch that makes education about cognitive bias so much less effective than it ought to be.
The Awareness Gap is the structural mismatch at the centre of cognitive bias in clinical decision making: biases operate in System 1 processing, which is automatic and fast, while awareness of those biases is a System 2 activity, which is deliberate and slow. By the time awareness can act, the biased judgment has already formed.
What does the research on debiasing interventions actually show?
If the Awareness Gap is structural, the most direct test of it is to look at what happens when clinicians are formally taught about cognitive bias and given tools to counteract it. The evidence from that body of research is more sobering than most training programmes acknowledge.
A systematic review by^† examining all available educational initiatives designed to reduce cognitive bias in clinical diagnosis, published across peer-reviewed and preprint sources, found that while all three major categories of debiasing intervention showed some promise in controlled conditions, none had been tested in real clinical settings, all reported instances of ineffectiveness, and none had measured long-term outcomes. The reviewers concluded that the usability and actual effectiveness of each intervention in practice remained unclear. This matters because the gap between a controlled educational exercise and a working emergency department is precisely where cognitive biases have their strongest effects.
Pat Croskerry, whose work on cognitive error in clinical practice has defined much of this field, proposed a universal model of diagnostic reasoning that explicitly accounts for how affective and environmental factors interact with cognitive processes (Academic Medicine, 2009; doi:10.1097/ACM.0b013e3181ace703). Croskerry's model identifies what he calls cognitive predispositions to respond: stable patterns in how clinicians process clinical information that persist across contexts and resist interruption by awareness alone. His position, supported by two decades of research, is that reducing diagnostic error requires structural changes to clinical environments, not just educational interventions aimed at individual reasoning.
Norman and colleagues, in their 2017 Academic Medicine paper on the causes of errors in clinical reasoning (doi:10.1097/ACM.0000000000001421), reached a finding that complicates the picture further. Cognitive bias alone is not the primary driver of diagnostic error. Knowledge deficits, where the clinician does not have the right illness script in their pattern library, account for a substantial proportion of mistakes that get attributed to bias. A clinician who appears to be anchoring on the wrong diagnosis may be anchoring correctly on the only diagnosis their pattern library makes available. The implication is that awareness training addresses a secondary cause while the primary cause goes unexamined.
Why do cognitive forcing strategies fail to override cognitive bias in real clinical conditions?
Cognitive forcing strategies are the most commonly recommended practical tool for cognitive bias in clinical decision making. The principle is that if clinicians can be trained to pause at key decision points and consciously consider alternative explanations before committing to a diagnosis, System 2 can review and potentially override what System 1 has produced. In theory this is sound. In practice it fails under the conditions where it is most needed.
Sherbino and colleagues conducted a controlled trial of cognitive forcing strategies designed specifically to overcome availability bias and search satisficing. They found no long-term effect. The AAFP literature review on flaws in clinical reasoning reached the same conclusion: interventions to reduce diagnostic error remain speculative, and no fail-safe approach exists. These findings are not surprising once the structural reasons are named.
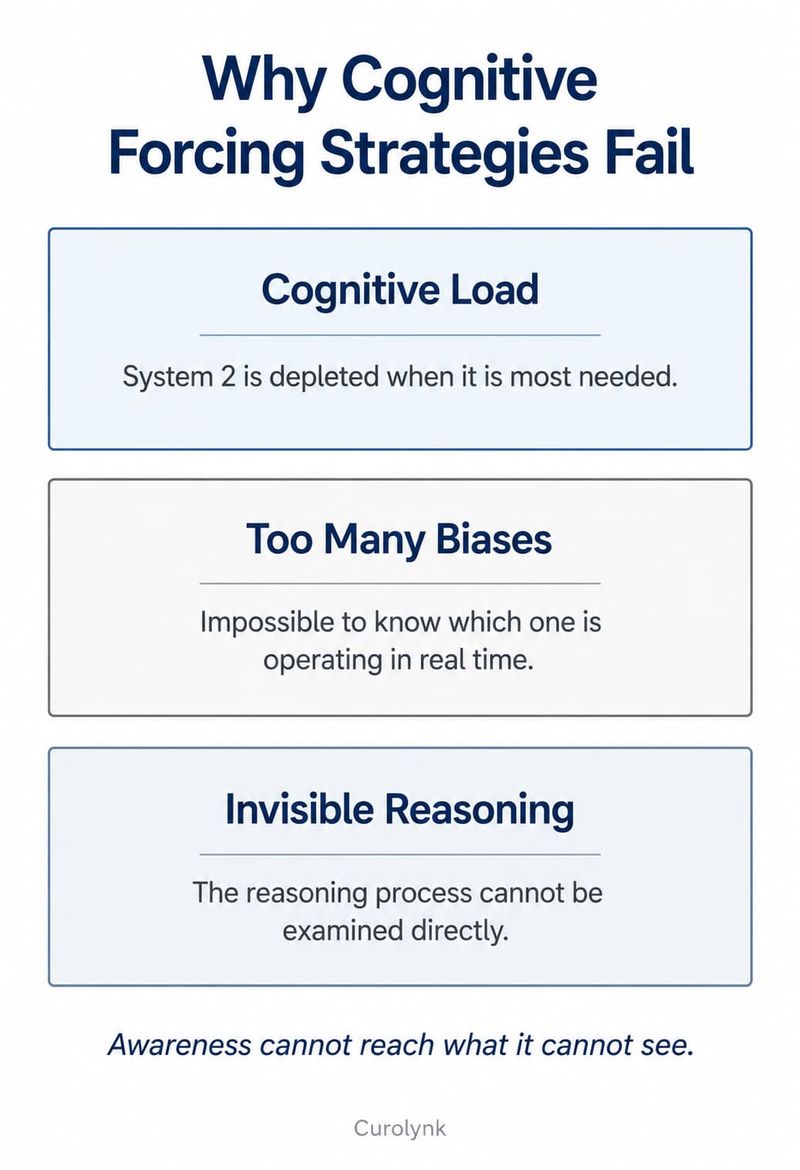
The first structural reason is cognitive load. Real clinical environments involve simultaneous demands on attention, time pressure, emotional weight, and frequently sleep deprivation. These are precisely the conditions under which System 2 is most depleted. Telling a clinician to slow down and deliberately check their reasoning is advice that is hardest to follow when it is most needed.
The second is that checking for bias requires knowing which bias to check for. More than 100 cognitive biases affecting clinical reasoning have been documented. Even a clinician who has memorised the taxonomy faces an impossible meta-cognitive task in real time: which bias is operating now, in this case, at this moment? The act of searching for the answer is itself subject to bias. Confirmation bias, for example, shapes not just the clinical diagnosis but the self-assessment of whether one is reasoning correctly.
The third is the invisibility of the reasoning process itself. Clinical reasoning, like clinical intuition, is substantially tacit, as explored in the framework described in why clinical intuition is hard to teach. The process that generates a diagnostic impression is not transparently available to the clinician generating it. A cognitive forcing strategy asks a clinician to examine a process they do not have direct access to. It can catch the output of reasoning. It rarely catches the mechanism.
What actually changes clinical decision making, and what does that mean for how clinicians train?
The research points toward two conclusions that the evidence supports more clearly than training systems currently reflect.
The first is that improving diagnostic accuracy is more reliably achieved by building a richer and more accurate pattern library than by teaching clinicians to catch biases in real time. Norman and colleagues' analysis found that when diagnostic errors attributed to cognitive bias were examined carefully, many were better explained by missing or inaccurate illness scripts. A clinician cannot recognise a presentation they have never encountered, and no amount of bias awareness compensates for a pattern that is absent. Deliberate, structured exposure to a wide range of clinical presentations, with corrective feedback that reinforces accurate pattern formation, does more for diagnostic accuracy than debiasing education.
The second is that structured reflection after the fact is more consistently effective than attempted real-time interruption. The AMA analysis of cognitive interventions found that guided reflection, reviewing diagnostic reasoning after a case has resolved, showed the most consistent positive outcomes across studies. This is consistent with the dual process
framework: post-case reflection is lower-stakes, lower-load, and gives System 2 a genuine opportunity to examine what System 1 produced without the pressure that made real-time interruption impossible. It does not prevent the next biased judgment. Over time, it reshapes the pattern library so that the next System 1 response is more accurate.
For medical educators this reframes the task. The question is not how to teach clinicians to catch biases in the moment. It is how to design training that builds richer illness scripts through structured exposure, and how to make reflective practice a routine feature of clinical culture rather than an occasional educational exercise. These are problems of exposure design and cultural design, not problems of individual awareness.
Curolynk is a platform built around the principle that clinical knowledge develops through structured peer interaction, not through individual study alone. The way the platform approaches cognitive bias in clinical decision making follows directly from what the research shows: that the conditions which build accurate clinical judgment are relational and contextual, not informational. Peer discussion of real cases, with the reasoning made explicit and examined, is closer to the reflective practice that the evidence supports than any individual debiasing exercise.
The Awareness Gap does not close through more awareness. It closes through better illness scripts, built through structured exposure to varied clinical presentations with corrective feedback, and through reflective practice embedded in clinical culture rather than delivered as a curriculum event. That is a different design task from what most training systems are currently built to perform. Naming the gap accurately is the necessary first step toward building something more useful.
Frequently asked questions
What is the most common cognitive bias in clinical decision making?
Anchoring bias, confirmation bias, and availability bias are consistently identified as the most frequently documented in clinical settings. Research examining emergency medicine found that overconfidence was present in approximately 22.5 percent of physician-reported diagnostic errors, making it the single most common cognitive bias contributing to mistakes in that setting. In practice, multiple biases operate simultaneously and are difficult to separate from one another.
Can cognitive bias in clinical decision making be meaningfully reduced?
The current evidence suggests it can be reduced, though not eliminated, through structural rather than individual approaches. Building richer illness scripts through deliberate exposure, embedding guided reflective practice after cases, and designing clinical environments that reduce cognitive load have the strongest evidence base. Awareness training alone, without these structural conditions, has not demonstrated durable effects in real clinical contexts.
Why do experienced clinicians still make bias-related diagnostic errors?
Because expertise and susceptibility to cognitive bias are not opposites. Experienced clinicians are faster and more accurate than novices precisely because their System 1 pattern libraries are larger and better calibrated. But the same automation that makes their reasoning fast also makes it less transparent to themselves and more difficult to interrupt. In some domains, expert System 1 processing is more susceptible to certain biases, particularly anchoring, because the initial impression forms so rapidly and with such confidence that it is rarely questioned.
References
- Kahneman, D. (2011). Thinking, Fast and Slow. Farrar, Straus and Giroux. Dual process theory, System 1 and System 2 framework. No DOI (book).
- Croskerry, P. (2002). Achieving quality in clinical decision making: cognitive strategies and detection of bias. Academic Emergency Medicine, 9(11), 1184-1204. doi:10.1197/aemj.9.11.1184. PubMed ID: 12414468.
- Croskerry, P. (2009). A universal model of diagnostic reasoning. Academic Medicine, 84(8), 1022-1028. doi:10.1097/ACM.0b013e3181ace703. PubMed ID: 19638921.
- Norman, G.R., Monteiro, S.D., Sherbino, J., Ilgen, J.S., Schmidt, H.G., and Mamede, S. (2017). The causes of errors in clinical reasoning: cognitive biases, knowledge deficits, and dual process thinking. Academic Medicine, 92(1), 23-30. doi:10.1097/ACM.0000000000001421. PubMed ID: 27782919.
- Sherbino, J., Kulasegaram, K., Howey, E., and Norman, G. (2014). Ineffectiveness of cognitive forcing strategies to reduce biases in diagnostic reasoning: a controlled trial. Canadian Journal of Emergency Medicine, 16(1), 34-40. doi:10.2310/8000.2013.130860. PubMed ID: 24424382.
- Saposnik, G., Redelmeier, D., Ruff, C.C., and Tobler, P.N. (2016). Cognitive biases associated with medical decisions: a systematic review. BMC Medical Informatics and Decision Making, 16(1), 138. doi:10.1186/s12911-016-0377-1. PMC5093937.
- Graber, M.L., Franklin, N., and Gordon, R. (2005). Diagnostic error in internal medicine. Archives of Internal Medicine, 165(13), 1493-1499. doi:10.1001/archinte.165.13.1493. PubMed ID: 16009864.
- Committee on Diagnostic Error in Health Care, National Academies of Sciences, Engineering, and Medicine. (2015). Improving Diagnosis in Health Care. National Academies Press. doi:10.17226/21794.