Why clinical intuition is hard to teach

Why clinical intuition is hard to teach, not just hard to explain
Why clinical intuition is hard to teach is a structural problem, not a communication one. The knowledge behind it cannot be put into words. Not because clinicians lack self-awareness. Because the kind of knowing that makes a great clinician is the kind that stops being accessible to conscious description once it becomes expertise.
Every senior doctor has watched a trainee struggle with something that feels, to them, completely obvious. The harder question has never been what to say. It has been why saying it rarely helps.
Clinical intuition is not a shortcut around reasoning. It is what reasoning becomes after enough repetition that the steps disappear and the conclusion arrives first.
Why is clinical intuition hard to teach when the clinician clearly knows what they know?
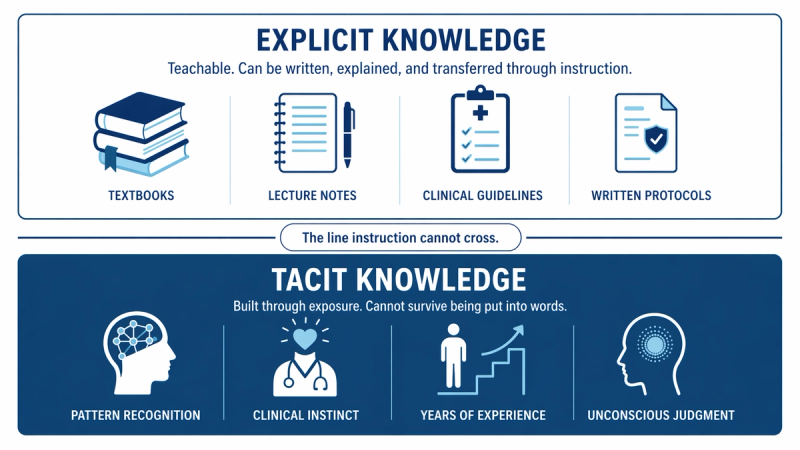
The answer sits in a distinction the philosopher Michael Polanyi named the Tacit Knowledge Model: the difference between knowing that and knowing how. Explicit knowledge can be written down and transmitted. Tacit knowledge is built through experience and cannot survive being translated into instruction. Polanyi's phrase 'we know more than we can tell' is not a metaphor. It describes a structural property of expert knowledge.
Clinical intuition is hard to teach because the knowledge behind it is tacit, not explicit. Tacit knowledge builds through repeated exposure and becomes compressed into pattern recognition. Once that compression happens, the intermediate steps are no longer available to the clinician to report. The explanation they give is honest. It is also incomplete.
When a senior clinician watches a registrar struggle and offers an explanation, both parties believe the explanation is the thing being transferred. It is not. What the senior clinician is transferring is the verbal account of a process they no longer have access to. The actual knowledge is in the pattern library they built over years of exposure. That library is not accessible through language.
What does the cognitive science of expertise say about how clinical judgment actually develops?
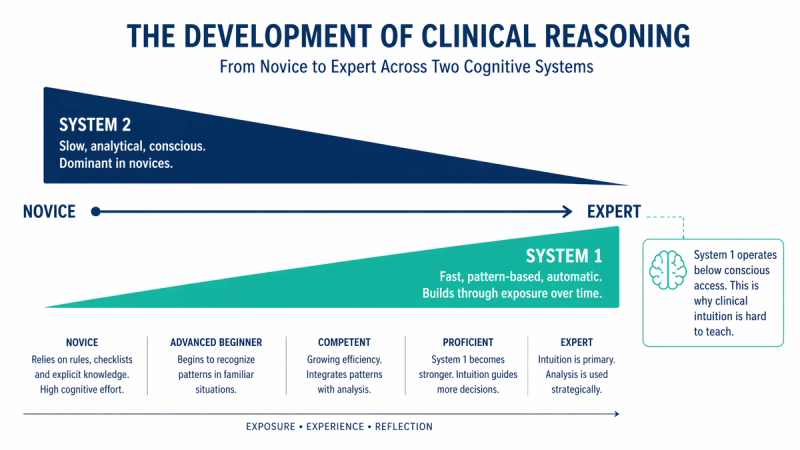
Gary Klein's Recognition-Primed Decision Model describes how experienced practitioners in high-stakes domains make decisions. The model found that experts do not evaluate options analytically under pressure. They recognise a situation as belonging to a known pattern and generate a course of action directly. The recognition is not conscious. It is the output of a pattern library built through thousands of real exposures.
This has a direct implication for clinical teaching. The thing that makes a senior clinician good at reading a deteriorating patient before the numbers move, or at recognising the atypical presentation that breaks the textbook rule, is not knowledge that was ever stored in an instructable form. It was built through exposure, reinforced through feedback, and is now operating below the level of voluntary access.
A study of expert and novice clinical reasoning by Eva et al. (2007), published in Medical Education, found that expert clinicians were significantly less likely than novices to use step-by-step analytical reasoning in diagnostic tasks. Not because they had abandoned reasoning, but because experience had automated it past the point of voluntary reporting. The expert demonstrating their reasoning process is demonstrating something different from the process they are actually using.
Why are the most experienced clinicians often the least effective at teaching this specific thing?
There is a paradox in clinical expertise that does not get named clearly enough. The deeper the intuitive knowledge, the less access the expert has to the process that built it. The clinician who cannot tell you how they knew the patient was going to deteriorate is not being evasive. They have genuinely lost the intermediate steps.
The pedagogical problem compounds when the expert, unable to articulate the process, concludes that the trainee simply needs more exposure or more effort. The explanation given is honest. The trainee receives it as complete. Neither party recognises that what was transmitted was a description of a destination, not a map of the route.
This is not a failure of teaching skill. It is a predictable consequence of what expertise does to the expert. The more automated the knowledge, the more invisible the mechanism that built it. The best clinical teachers are often not the ones with the deepest intuition. They are the ones who retain enough memory of building it to design conditions in which trainees can build their own.
What can actually be done if explanation cannot transfer clinical intuition?
The answer is to stop treating it as a content transfer problem and start treating it as an exposure design problem. The conditions that build clinical intuition are reasonably well understood. Deliberate practice with meaningful variation in case complexity. Immediate and corrective feedback. Repeated exposure to the full range of presentations of a given clinical situation. Enough volume that the pattern library builds through reinforcement.
The senior clinician's role in this is not primarily verbal. It is curatorial. The most valuable thing they can do for a trainee is select the right cases, at the right moment of complexity, with the right feedback loop in place. That is a different job description from lecturer. Most training structures do not explicitly design for it.
At Curolynk, the framework for understanding why knowledge does or does not transfer between clinicians starts here. The gap between what a senior clinician knows and what a trainee can receive through instruction is not a gap that better explanation closes. It is a gap that only structured exposure over time can close. Recognising which gap you are looking at is where more useful decisions begin.
The framework does not make the gap easier to close. It makes it harder to blame the wrong things for why it exists. Once you stop blaming the explanation, you can start designing the conditions. That is usually the more useful place to be.
References
- Croskerry, P. (2009). A universal model of diagnostic reasoning. Academic Medicine, 84(8), 1022-1028. Available via PubMed.
- Eva, K.W., Hatala, R.M., LeBlanc, V.R., and Brooks, L.R. (2007). Teaching from the clinical reasoning literature: combined reasoning strategies help novice diagnosticians overcome misleading information. Medical Education, 41(12), 1152-1158. PubMed ID: 18045367.
- Klein, G. (1998). Sources of Power: How People Make Decisions. MIT Press. Recognition-Primed Decision Model.
- Norman, G. (2009). Dual processing and diagnostic errors. Advances in Health Sciences Education, 14(S1), 37-49. Available via PMC.
- Polanyi, M. (1966). The Tacit Dimension. University of Chicago Press. Tacit Knowledge Model. Page 4: 'we can know more than we can tell.'