Why clinical knowledge decays, and what that means for expertise.

Clinical knowledge decay is not a failure of memory. It is a structural narrowing that accelerates quietly through the middle years of a clinical career and is almost never named as the thing it actually is.
Every senior clinician has areas of practice they once knew deeply and no longer reach for. The knowledge did not disappear overnight. It receded gradually, replaced by the narrower and more frequently used expertise that specialisation demands. The question worth asking is not whether this happens, but what it means for how a clinician understands the knowledge they still have.
The clinician who has practised longest in a narrow field has not accumulated knowledge across a career. They have traded breadth for depth, and the breadth they traded away is gone.
What does clinical knowledge decay actually mean, and how is it different from forgetting?
The term most relevant here is disuse atrophy, applied to knowledge rather than to muscle. Researchers studying knowledge retention in medical trainees use this term to describe what happens when foundational knowledge is no longer actively engaged after training moves into more specialised territory. The mechanism is the same one Hermann Ebbinghaus described in 1885 with his forgetting curve: unused knowledge degrades rapidly at first and then flattens, with the final level of retention determined largely by how deeply the knowledge was encoded and how often it has been reactivated since.
But clinical knowledge decay is not simply about forgetting facts. The more significant loss is in the tacit layer: the pattern recognition and clinical judgment built through repeated exposure to a particular type of case. A physician who trained as a generalist and then specialised in cardiology does not merely forget dosing tables for conditions they no longer treat. They lose the finer clinical read on presentations in those areas, the calibration that only comes from seeing a particular pattern hundreds of times. That calibration does not survive disuse.
Clinical knowledge decay is the process by which clinical skills and judgment in areas that are no longer actively practised degrade over time. It is distinct from forgetting facts, because the knowledge most affected is tacit: the pattern recognition built through repeated clinical exposure that cannot be recovered through revision alone.
This distinction matters because it changes what is actually at stake. Forgetting a fact is recoverable. A clinician can look it up. Losing the tacit judgment that contextualises a clinical presentation is a different kind of loss, and it is not recoverable through a refresher course.
Why does specialisation accelerate clinical knowledge decay rather than prevent it?
The assumption most clinicians carry is that more years of practice means more knowledge. This is true within the domain of specialisation. It is not true across the full range of a clinician's earlier training. Specialisation creates a feedback structure in which the knowledge that is used daily becomes more refined, and the knowledge that is not used begins to thin.
A 2024 study published in ATS Scholar examined knowledge of core physiological concepts among critical care fellows, clinicians who had completed medical school and residency and were now in subspecialty training (doi:10.34197/ats-scholar.2024-0036OC). It found that foundational knowledge from medical school had decayed substantially, with fellows frequently unable to access concepts that their training had assumed were retained. The researchers noted that educators often assume trainees carry foundational knowledge forward into advanced training. The study found this assumption to be frequently wrong.
Research examining surgical residents who took dedicated research breaks found that both faculty and residents perceived the largest skill reduction in complex procedures and clinical judgment tasks, precisely the areas where tacit knowledge is most essential and most vulnerable to disuse (D'Angelo et al., Journal of Surgical Research, 2015; PMC4604038). The knowledge that degrades fastest under disuse is not the knowledge that was most superficially held. It is often the knowledge that was hardest to build in the first place.
This creates a quiet paradox in clinical careers. The deeper a clinician's expertise in one domain, the more their knowledge has been shaped by what they chose to focus on and what they left behind. The most experienced cardiologist in a hospital may have a narrower clinical knowledge base than a fourth-year resident, not in their specialty, but across the full range of medicine they once knew. Specialisation is a trade. Most clinicians make it without recognising what they are trading.
What does clinical knowledge decay mean for how a clinician should understand their own expertise?
The most immediate implication is one of accuracy. A clinician who trained broadly and then specialised is not the same clinician in the areas outside their specialty that they were ten years ago. This is not a comfortable thought, and it is rarely surfaced directly. It tends to emerge in the quiet hesitation before a clinical question outside the specialty, the moment where a clinician reaches for a certainty that used to be there and finds something less solid.
There is a second implication for teaching. The knowledge a senior clinician draws on when teaching trainees is the knowledge they have been actively using. The knowledge they have not been using has decayed. This means the picture of medicine that a very experienced specialist paints for their trainees is filtered through decades of selective activation, shaped as much by what the specialist stopped engaging with as by what they continued to develop. The senior clinician is not just unable to make tacit knowledge explicit, as the framework in why clinical intuition is hard to teach describes. They may also be working from a narrower version of the knowledge they once had.
A 2024 systematic review in BMC Medical Education examined retention and application of basic sciences among practising physicians across multiple career stages (Albert et al., BMC Med Educ 24:997, doi:10.1186/s12909-024-05952-8). It found that active use of knowledge was the most consistent predictor of retention. Clinicians who continued to engage with foundational concepts through teaching, research, or clinical breadth retained significantly more than those who had narrowed into single-domain practice. The review noted that years of experience and knowledge breadth are not positively correlated and should not be assumed to be.
What changes when clinical knowledge decay is named rather than ignored?
Most clinical training systems treat the knowledge a doctor acquired in medical school and residency as a permanent foundation. Continuing medical education is typically structured around updating a clinician on new developments in their area of practice, not on actively maintaining the broader base that specialisation has been slowly withdrawing from.
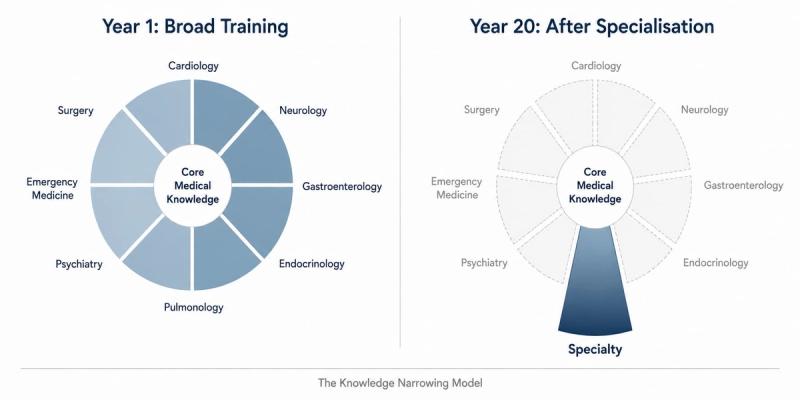
It is useful to name this as a framework rather than a problem: the Knowledge Narrowing Model. The model holds that clinical expertise does not expand linearly across a career. It deepens in the direction of active use and recedes in the direction of disuse. The shape of a clinician's knowledge at year twenty of practice is not a wider version of their knowledge at year five. It is a different shape, with different depths and different gaps, formed by decades of selective engagement.
Acknowledging this as a structural feature of clinical careers, rather than a personal failing or a problem of ageing, changes the question. The question is no longer whether a clinician's knowledge is deteriorating in certain areas. It is whether they have any deliberate relationship with that deterioration, and whether their practice creates conditions for the knowledge that still matters to be maintained.
For the educator, the implication is specific. A clinician who teaches regularly has a mechanism for knowledge maintenance that their peers who only practise do not. Teaching requires articulating reasoning that clinical practice often allows to remain implicit. It requires returning to foundational concepts to explain them. This is one of the structural reasons why clinicians who teach tend to retain broader knowledge across longer careers than clinicians who do not. The teaching is doing work that specialised clinical practice is not.
At Curolynk, the recognition that clinical knowledge is not a static archive, that it is actively maintained by use and actively depleted by disuse, is foundational to how the platform thinks about knowledge transfer between clinicians. The conversation between a senior specialist and a junior doctor is not just a transfer of what the senior knows. It is, structurally, an act of maintenance for both of them.
Clinical knowledge decay does not resolve itself. The Knowledge Narrowing Model does not offer a solution to that. What it offers is a more accurate account of what expertise actually looks like across a career, which is the necessary starting point for any clinician who wants to understand not just what they know, but what they no longer do.
References
- Custers, E.J.F.M. (2010). Long-term retention of basic science knowledge: a review study. Advances in Health Sciences Education, 15(1), 109-128. doi:10.1007/s10459-008-9101-y. PubMed ID: 18274876.
- Albert, F.A., Seidu, A.A., Mason, H.M., Anderson, E., Alele, F.O., Heggarty, P., et al. (2024). A systematic review of medical practitioners' retention and application of basic sciences to clinical practice. BMC Medical Education, 24(1), 997. doi:10.1186/s12909-024-05952-8. PMC11396528.
- Decay in Physiologic Knowledge since Medical School among Critical Care Fellows (DIP Study). ATS Scholar, 2024. doi:10.34197/ats-scholar.2024-0036OC.
- D'Angelo, A.D., et al. (2015). Residents' perception of skill decay during dedicated research time. Journal of Surgical Research, 199(1), 25-34. doi:10.1016/j.jss.2015.07.015. PMC4604038.
- Ebbinghaus, H. (1885/1913). Memory: A Contribution to Experimental Psychology. Teachers College, Columbia University. Foundational forgetting curve research on knowledge retention over time.