what gets lost when senior doctors teach

What gets lost when senior doctors teach, and why effort has nothing to do with it
What gets lost when senior doctors teach is not the information they intended to share. The information arrives. What does not arrive is the layer of knowledge underneath it. That layer is built through years of clinical exposure and now operates below the level of conscious description.
The senior doctor is not withholding anything. They are teaching at full effort. The problem is not how much they give. It is that the most important part of what they know is not available to them to give.
When a senior doctor teaches, what crosses the gap is the account of their knowledge, not the knowledge itself, and the difference between the two is the size of the gap their trainee will spend years trying to close.
What exactly gets lost when senior doctors teach, and why cannot explanation recover it?
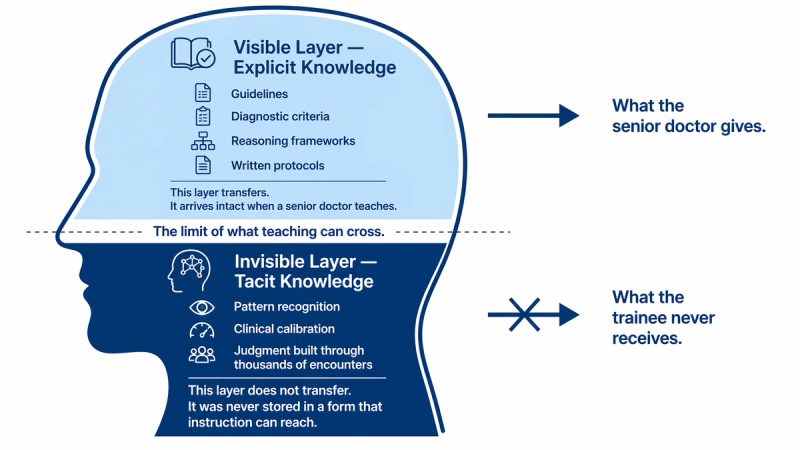
The knowledge that makes a senior clinician exceptional is stored in two layers. The first layer is explicit: the guidelines, the diagnostic criteria, the reasoning frameworks they can write down and explain. This layer transfers through teaching. It arrives intact.
The second layer is tacit: the pattern recognition built through thousands of clinical encounters, the calibration of what feels right before the data confirms it, the judgment that cannot be reduced to a rule. Michael Bereiter and Marlene Scardamalia described this divide in their work on expert knowledge as the difference between formal knowledge and the embedded practical understanding that governs how experts actually function. Formal knowledge can be taught. The embedded layer cannot be handed across. It has to be built.
What gets lost when senior doctors teach is the tacit layer of clinical knowledge. This layer builds through repeated exposure and compresses into automatic judgment. Once compressed, it is no longer accessible to conscious description. The senior doctor gives everything they have access to. What they cannot access, they cannot give.
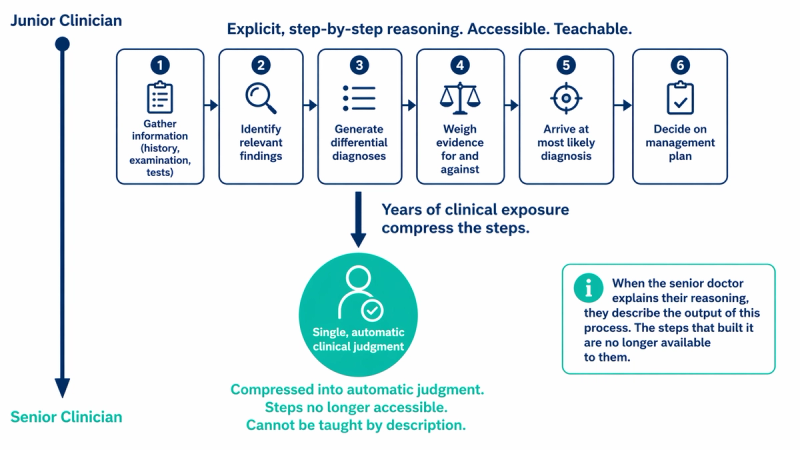
The trainee watching a senior clinician make a rapid, accurate judgment and then explain it is watching two different events. The judgment came from the tacit layer. The explanation came from the explicit layer. The explanation is accurate as a description of the conclusion. It is not a description of the process that produced it. That process is what the trainee needs most, and it is precisely what cannot be recovered through explanation.
Why does this happen even when the senior doctor is a committed and experienced teacher?
The mechanism behind this failure was described by Michael Eraut in his 2000 research on non-formal learning in the workplace. Eraut identified that expert practitioners develop what he called non-formal knowledge, understanding that is acquired through practice and becomes so integrated into routine performance that the practitioner is no longer aware of using it. This is not laziness or poor communication. It is the natural consequence of what prolonged expertise does to knowledge.
The better a clinician becomes, the more their knowledge automates. The more it automates, the less access they have to the process that built it. A consultant who has assessed a thousand patients with a specific presentation no longer consciously runs through the steps. They arrive at an impression. When they try to teach from that impression, they describe its conclusion. They cannot describe its mechanism, because the mechanism is no longer a sequence of conscious steps. It is a single response.
This means that the most experienced clinicians are, in a very specific sense, the least equipped to teach the thing that makes them most valuable. Not because they are poor teachers, but because the depth of their expertise has placed the most important part of it beyond their own reach. This is the same structural problem explored in Why clinical intuition is hard to teach, which addresses why clinical intuition specifically resists direct instruction. The transfer failure here is the broader version of that same mechanism.
What does the trainee actually receive, and what are they left to build on their own?
From the trainee side, the experience of receiving teaching from a senior doctor is often described as valuable but incomplete. The information given is correct. The reasoning offered is coherent. But there is frequently a gap between what was explained and what the trainee can replicate in the next encounter. They were given the map. They were not given the territory.
Bolander Laksov, Lonka, and Josephson (2008), in a study of medical teachers at Karolinska Institutet, found that most clinical teachers recognised that knowledge transfer was a problem but had no formal strategy for addressing it. The teaching they offered was driven by their own experience of how they had learned, which was largely through exposure, not instruction. The advice most commonly given to trainees, to see more patients and to pay attention, reflects this accurately. It is the honest answer. It is also an admission that formal teaching cannot close the gap.
What the trainee is left to build on their own is the tacit layer, through accumulated experience over time. The explicit layer they received through teaching gives them the vocabulary and the framework to make sense of what they observe. But the pattern library that will eventually allow them to function as a senior clinician builds only through repeated exposure to real clinical situations, with enough variation and feedback that the right patterns get reinforced. That process cannot be shortcut through better explanation. It can only be accelerated through better exposure design.
What changes when the teaching relationship is understood this way?
When the gap is correctly named as structural rather than personal, the teaching relationship changes in two directions at once. The senior doctor is released from the assumption that better explanation would close it. The trainee is released from the assumption that their difficulty keeping up reflects insufficient effort or attention.
The more productive question becomes not how to explain more clearly, but how to design better conditions for the tacit layer to build. That means thinking about which cases a trainee encounters, in what sequence, at what level of complexity, and with what kind of feedback attached. It means recognising that the senior doctor's most valuable contribution to a trainee is not verbal. It is curatorial.
At Curolynk, this distinction between what can be taught and what can only be built through exposure is foundational to how the platform thinks about knowledge transfer between clinicians. The gap is not a failure of teaching. It is a property of the knowledge. Understanding that shifts the question from why the teaching is not working to what conditions are actually needed for the knowledge to develop.
For the trainee, this reframing changes something important. The years of clinical exposure ahead are not remediation for a gap the teaching should have closed. They are the mechanism. The teaching gave the framework. The exposure builds the knowledge the framework is for. Understanding the difference is the first step in using both more deliberately.
References
- Bereiter, C. and Scardamalia, M. (1993). Surpassing Ourselves: An Inquiry into the Nature and Implications of Expertise. Open Court Publishing. Formal knowledge vs embedded informal knowledge and skill.
- Bolander Laksov, K., Lonka, K., and Josephson, A. (2008). How do medical teachers address the problem of transfer? Advances in Health Sciences Education, 13(3), 345-360. PubMed ID: 17203269.
- Eraut, M. (2000). Non-formal learning and tacit knowledge in professional work. British Journal of Educational Psychology, 70(1), 113-136. Available via Wiley Online Library.